

TS. PHẠM HỮU VĂN
11.2 Rối loạn nhịp bộ nối nhĩ thất
11.2.1 Nhịp nhanh vào lại nút nhĩ thất (AVNRT)
AVNRT dùng để chỉ sự vào lại trong khu vực của nút nhĩ thất (AVN), nhưng vòng chính xác vẫn còn khó xác định. AVN là cấu trúc ba chiều với độ biến thiên lớn hơn trong tính liên tiếp của tổ chức không gian và khả năng kết nối khoảng cách kém do biểu hiện khác biệt của các đồng dạng connexin, các điều kiện đưa ra sự giải thích cho dẫn truyền kép và gây rối loạn nhịp vào lại tại nút. [312–314] Cũng đã có bằng chứng tổ chức và điện sinh học có thể được xem xét các phần phụ thuộc bên phải và dưới trái của AVN ở người, và các đường vào nhĩ nút dễ dàng, có thể cung cấp nền giải phẫu cho đường chậm. [315,316] Do đó, các mô hình toàn diện của vòng nhịp nhanh cho tất cả các hình thái của AVNRT trên cơ sở khái niệm của các đường vào nhĩ nút đã được đưa ra. [47.317]
Khởi phát AVNRT dường như để xuất hiện theo hai phương thức theo thời gian. Ở nhiều bệnh nhân, các cơn rối loạn nhịp biểu hiện thực sự sớm trong cuộc đời, trong khi ở một tỷ lệ đáng kể bệnh nhân AVNRT bắt đầu muộn hơn, ví dụ: trong thập kỷ thứ tư hoặc thứ năm của đời sống. [318] Một nửa số bệnh nhân có các triệu chứng tối thiểu và các cơn nhịp nhanh, không thường xuyên có thể trở nên không có triệu chứng trong vòng 13 năm tiếp theo. [319] AVNRT có thể dẫn đến AF mà thông thường, mặc dù không phải lúc nào cũng không thay đổi, được loại bỏ sau triệt phá AVNRT qua catheter. [320] AVNRT gia đình nên được xem xét. [321]
11.2.1.1 Chẩn đoán
ECG 12 chuyển đạo trong quá trình nhịp nhanh
Thông thường, AVNRT là nhịp nhanh phức bộ hẹp, tức thời gian QRS <120 ms, trừ khi có sự dẫn truyền bất thường, thường là dạng RBBB, hoặc tồn tại khiếm khuyết dẫn truyền trước đó (Hình 13). Sự phân ly AV đặc biệt không phổ biến, nhưng nó có thể xảy ra vì cả tâm nhĩ và tâm thất đều không cần thiết cho vòng vào lại. Do đó, cùng tồn tại với AF hoặc block dẫn truyền có thể nhưng hiếm. [66.322] Đoạn ST chênh xuống có thể được nhìn thấy trong hoặc sau nhịp nhanh.
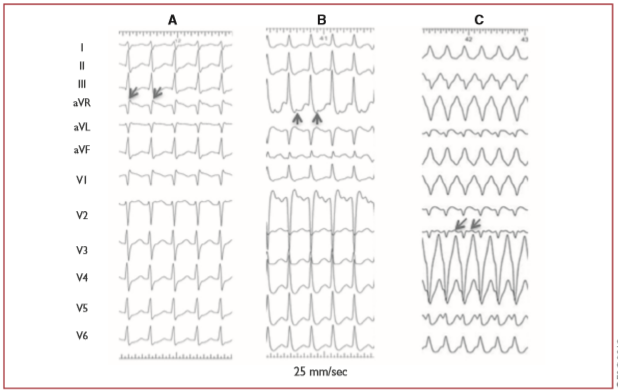
Hình 13. Nhịp nhanh vào lại tại nút nhĩ thất. (A) Nhịp nhanh vào lại tại nút nhĩ thất điển hình. (B) Nhịp nhanh vào lại nút nhĩ thất không điển hình. (C) AVNRT không điển hình với (ít gặp) dẫn truyền lệch hướng block nhánh bó trái. Các sóng P ngược được chỉ bằng các mũi tên.
Ở hình thái AVNRT điển hình (còn được gọi là AVNRT chậm nhanh), sóng P ngược có liên quan đến QRS và, trong phần lớn các trường hợp, không thể phát hiện được hoặc rất gần với phức hợp QRS. Do đó, sóng P hoặc bị phức bộ QRS che lấp hoặc được xem như một sóng P’ kết thúc nhỏ không có trong nhịp xoang. [323]
Ở hình thái AVNRT không điển hình, sóng P có thể nhìn thấy rõ trước QRS, tức là RP > PR, biểu hiện nhịp nhanh RP dài và âm hoặc nông ở các chuyển đạo II, III, aVF và V6, nhưng dương ở V1. .[317]
Sự chênh xuống của đoạn ST liên quan đến nhịp nhanh, sự biến đổi của khoảng RR, cũng như các thay đổi luân phiên của QRS cũng có thể được nhìn thấy. Đặc biệt, mặc dù độ nhạy cảm khiêm tốn, tiêu chuẩn ECG cho AVNRT, trái ngược với AT và AVRT, là sự xuất hiện sóng R giả (pseudo S wave) ở chuyển đạo V1 và sóng S giả (pseudo S wave) ở các chuyển đạo dưới, chẽ đôi ở aVL, và R giả ở aVR. [45] Nếu nhịp nhanh được khởi đầu bằng các nhắt bóp nhĩ ngoại vị, sóng P khởi đầu (ngoại vị) thường khác với các sóng P tiếp theo (ngược).
Nghiên cứu điện sinh lý
Sự không đồng nhất của cả hai mẫu dẫn truyền nhanh và chậm đã được mô tả rõ ràng và tất cả các dạng AVNRT có thể hiển thị các mẫu kích hoạt trước, sau và giữa hoặc thậm chí dẫn truyền ngược LA. [322 Led324] Do đó, các thủ pháp điện sinh lý chuyên biệt có thể được đòi hỏi cho chẩn đoán phân biệt AVRN điển hình, đặc biệt, không điển hình với AT ổ hoặc AVRT do đường vách ẩn. [45] Hình thái hiếm gặp của AT nhạy cảm với verapamil là do vào lại ở tổ chức nhĩ sát với AVN, nhưng không phải hệ thống dẫn truyền nút nhĩ thất. [325]
Nhịp nhanh vào lại nút nhĩ thất điển hình
Trong hình thái chậm nhanh của AVNRT, sự khởi đầu của kích hoạt nhĩ xuất hiện trước, lúc khởi đầu hoặc ngay sau phức hợp QRS, do đó duy trì tỷ lệ AH / His-nhĩ (HA) > 1. Khoảng VA được đo từ khi bắt đầu kích hoạt tâm thất trên ECG bề mặt đến độ lệch sớm nhất của kích hoạt tâm nhĩ trên điện đồ bó His là ≤60 ms. Mặc dù, kích hoạt tâm nhĩ ngược sớm nhất thường được ghi lại ở điện cực bó His, các nghiên cứu lập bản đồ cẩn thận đã chứng minh đường dẫn nhanh sau hoặc thậm chí vách trái có thể xảy ra ở ≤7,6% ở bệnh nhân AVNRT điển hình. [326-328]
Nhịp nhanh vào lại nút nhĩ thất không điển hình
AVNRT không điển hình được thấy ở ∼6% của tất cả các trường hợp AVNRT, [317] ở một số bệnh nhân có thể cùng tồn tại với hình thái điển hình. [329] Tỷ lệ mắc AVNRT không điển hình cao hơn đã được ghi nhận ở các vận động viên. [330] Trong hình thái được gọi là AVNRT nhanh – chậm, các điện đồ nhĩ ngược bắt đầu rõ sau hoạt động thất với tỷ lệ AH/HA <1, cho thấy dẫn truyền ngược chậm hơn so với dẫn truyền xuôi. Khoảng AH <185 – 200 ms. Khoảng VA được đo từ khi bắt đầu kích hoạt tâm thất trên ECG bề mặt đến độ lệch sớm nhất của kích hoạt tâm nhĩ ở điện cực bó His > 60 ms. Kích hoạt tâm nhĩ ngược sớm nhất thường được báo cáo ở đáy tam giác Koch, gần xoang vành, nhưng nó có thể thay đổi, với kích hoạt tâm nhĩ lệch ở vách dưới hoặc thậm chí là xoang vành xa. [328.331.332] dạng chậm chậm, tỷ lệ AH / HA là> 1 và khoảng AH > 200 ms, nhưng khoảng VA là > 60 ms, cho thấy hai đường dẫn chậm được sử dụng cho cả kích hoạt xuôi và ngược. Kích hoạt tâm nhĩ ngược sớm nhất thường là ở lỗ xoang vành, nhưng các biến thể của kích hoạt ngược tâm nhĩ trái cũng đã được công bố. [333.334] Sự khác biệt giữa các hình thái ‘nhanh – chậm’ và ‘chậm – chậm’ không có ý nghĩa thực hành, một số trường hợp nhất định của AVNRT không điển hình không thể được phân loại theo các tiêu chuẩn đã được mô tả. [324] Ngoài ra còn có bằng chứng cho thấy con đường “nhanh” trong quá trình AVNRT chậm – nhanh không giống với thành phần “nhanh” của cái gọi là AVNRT nhanh – chậm. [329] Do đó, AVNRT có thể được phân loại là điển hình hoặc không điển hình theo khoảng HA, hoặc khi điện đồ bó His không được ghi lại một cách đáng tin cậy theo khoảng VA được đo trên điện cực ghi bó His. [322], Bảng 12 trình bày hệ thống phân loại quy ước. Các cách tiếp cận khác cũng đã được công bố. [335]
Bảng 12. Phân loại các type nhịp nhanh vào lại nút nhĩ thất [324]
| HA | VA (His) | AH/HA | |
| AVNRT điển hình | ≤70 ms | ≤60 ms | >1 |
| AVNRT không điển hình | >70 ms | >60 ms | Variable |
Nhịp nhanh vào lại nút nhĩ thất không điển hình đã được phân loại theo truyền thống như nhanh – chậm (His – nhĩ > 70 ms, thất nhĩ > 60, nhĩ – His / His – nhĩ <1 và nhĩ – His <200 ms) hoặc chậm – chậm (His – nhĩ > 70 ms, khoảng thất nhĩ > 60 ms, nhĩ – His / His – nhĩ > 1, và nhĩ – His > 200 ms). Các loại trung gian, không được phân loại cũng có thể tồn tại. AH = khoảng thời gian nhĩ – His; AVNRT = nhịp nhanh vào lại nút nhĩ thất; HA = Khoảng thời gian His – nhĩ; VA = khoảng thời gian thất – nhĩ được đo từ khởi đầu hoạt động của thất trên ECG bề mặt đến độ lệch sớm nhất của hoạt động của nhĩ trên điện đồ bó His.
11.2.1.2 Điều trị
Khuyến cáo điều chỉnh nhịp nhanh vào lại nút nhĩ thất (AVNRT)
| Khuyến cáo | Classa | Levelb |
| Điều trị cấp thời | ||
| Các bệnh nhân huyết động không ổn định | ||
| Chuyển nhịp đồng bộ DC được khuyến cáo cho các bệnh nhân không ổn định huyết động. [86-88] | I | B |
| Các bệnh nhân huyết động ổn đỉnh. | ||
| Thủ pháp phế vị, tốt hơn ở tư thế nằm với chân nâng lên cáo, được khuyến cáo. [41,89-91] | I | B |
| Adenosine (6-18 mg i.v. bolus) được khuyến cáo nếu thủ pháp phế vị thất bại. [92-94] | I | B |
| Verapamil hoặc diltiazem i.v. nên được xem xét nếu thủ pháp phế vị và adenosine thất bị. [92,94-98] | IIa | B |
| Beta-blockers (i.v. esmolol hoặc metoprolol) nên được xem xét nếu thủ pháp phế vị và adenosine thất bại. [97,99,100] | IIa | C |
| Chuyển nhịp đồng bộ DC được khuyến cáo khi điều trị thuốc thất bại để chuyển nhịp hoặc kiểm soát nhịp nhanh. [87,88] | I | B |
| Điều trị lâu dài | ||
| Triệt phá qua catheter được khuyến cáo cho AVNRT có triệu chứng, tái phát. [208,336-339] | I | B |
| Diltiazem hoặc verapamil, ở các bệnh nhân không có HFrEF, hoặc beta-blockers nên dược xem xét nếu triệt phá không được mong muons hoặc khả thi. [340-342] |
IIa |
B |
| Kiêng khỏi điều trị nên được xem xét để các bệnh nhân có triệu chứng tối thiểu với các cơn nhịp nhanh không thường xuyên, ngắn. [319] | IIa | C |
i.v. verapamil và diltiazem chống chỉ định khi huyết áp thấp hoặc HFrEF.
i.v. beta-blockers được chống chỉ định khi có suy tim mất bù.
DC = dòng điện một chiều; HF = suy tim; HFrEF = suy tim với phân suất tống máu giảm; i.v. = đường tĩnh mạch.
aClass khuyến cáo.
bMức độ bằng chứng.
11.2.1.2.1 Điều trị cấp thời
Hầu hết các dữ liệu về hiệu quả của các thủ pháp phế vị và adenosine để cắt cơn nhịp nhanh cấp thời được đưa ra từ các quần thể SVT hỗn hợp, như được mô tả trong phần 10.1.1 về điều trị cấp thời SVT nói chung, nhưng dường như chúng ít thành công hơn trong AVNRT so với AVRT. [89,90,102] Một liều diltiazem uống (120 mg) cộng với thuốc chẹn beta (ví dụ propranolol 80 mg) có thể chuyển nhịp được ≤ 94% bệnh nhân, nhưng có nguy cơ tụt huyết áp, block AV thoáng qua hoặc ngất hiếm gặp. [342.343] Cần thận trọng ở người cao tuổi và ở những bệnh nhân bị rối loạn dẫn truyền xoang hoặc nút AV. Một liều flecainide đường uống (3 mg / kg) cũng có thể có hiệu quả, mặc dù ở mức thấp hơn. [342.344] Intranasal etripamil có triển vọng (xem phần 10.1.1). [129] Hiếm khi, các thủ thuật cường phế vị và adenosine không thể cắt nhịp nhanh và nhịp tim nhanh và hạ huyết áp tiếp theo, chuyển nhịp DC đồng bộ được chỉ định [101] (Hình 14).
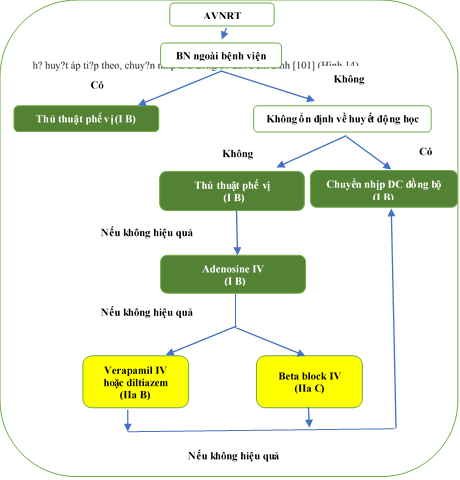
Hình 14. Điều trị cấp thời nhịp nhanh vào lại nút xoang. AVNRT = nhịp nhanh vào lại nút xoang; i.v. = đường tĩnh mạch. BN = bệnh nhân. DC = dòng điện một chiều.
11.2.1.2.2 Triệt phá qua catheter
Nghiên cứu lâm sàng ngẫu nhiên mới đây (RCT) đã so sánh triệt phá qua catheter như điều trị đầu tiên với bằng thuốc đã chứng minh lợi ích đáng kể trong nhập viện liên quan đến rối loạn nhịp.[336] Hơn nữa, triệt phá qua catheter cho SVT nói chung, và AVNRT nói riêng, là điều trị hiện nay để lựa chọn cho các bệnh nhân có triệu chứng do nó đã cải thiện đáng kể chất lượng sống [28,345,346] và giảm chi phí. [347–349] Thay đổi đường chậm có hiệu quả cho cả hai AVNRT điển hình và không điển hình.[338] Thông thường, phương pháp tiếp cận giải phẫu và lập bản đồ phối hợp được sử dụng, với các tổn thương triệt phá được đưa ra ở phần dưới tam giác Koch, hoặc từ phải hoặc bên trái vách. [337- 339.350.351] Cách tiếp cận này mang lại tỷ lệ thành công 97%, có tỷ lệ tái phát ∼1.3 – 4%, và có liên quan đến nguy cơ block AV <1% trong các báo cáo trước đây. [203,204,352,353] Kinh nghiệm gần đây cho thấy ở các trung tâm có kinh nghiệm, thủ thuật có thể được thực hiện ở cả AVNRT điển hình và không điển hình hầu như không có nguy cơ block AV, bằng cách nhắm mục tiêu mở rộng dưới nút và tránh vách giữa, vòm xoang vành. [208,338,354,355] Tỷ lệ thành công thấp hơn (82%) và nguy cơ block tim cao hơn (14%) ở bệnh nhân bị bệnh tim bẩm sinh trưởng thành (ACHD). [356] Thông thường, các đợt tái phát được ghi nhận thấy trong vòng 3 tháng sau thủ thuật thành công ở những bệnh nhân có triệu chứng gặp phải các cơn nhịp tim nhanh, [317,329,336,338] nhưng ở trẻ, ≤18 tuổi, tái phát có thể được ghi nhận thấy sau 5 năm sau khi triệt phá. [357] IST (nhịp xoang nhanh không phù hợp) có thể xảy ra, nhưng thường thoáng qua và không thường xuyên xảy ra sau quá trình triệt phá đường chậm. [358] Tuổi cao không phải là một chống chỉ định cho triệt phá đường chậm. [359] Block tim độ I tồn tại trước có nguy cơ cao hơn đối với block AV muộn và tránh triệt phá đường chậm mở rộng được ưu tiên trong các điều kiện như vậy.[360] Hầu như không có trường hợp tử vong liên quan đến thủ thuật. [11,13,203-205,208] Có nguy cơ block AV thấp hơn, nhưng có liên quan đến tỷ lệ tái phát cao hơn đáng kể. [361-363] Hồ sơ an toàn thuận lợi và tỷ lệ thành công lâu dài cao hơn ở bệnh nhân trẻ tuổi khiến đặc biệt hấp dẫn trong điều trị trẻ em. [364] AVNRT là một nguyên nhân gây ra những shock không phù hợp ở những bệnh nhân cấy máy khử rung tim (ICD) và, trong trường hợp thường xuyên, triệt phá qua catheter được chỉ định rõ ràng. [365]
11.2.1.2.3 Điều trị lâu dài
Bệnh nhân có các triệu chứng tối thiểu và các cơn nhịp nhanh ngắn không thường xuyên có thể được theo dõi không cần triệt phá hoặc điều trị thuốc lâu dài (Hình 15). Khoảng một nửa trong số họ có thể trở nên không triệu chứng trong vòng 13 năm tới. [319] Sử dụng thuốc chống loạn nhịp kéo dài làm giảm tần suất và khoảng thời gian của AVNRT, nhưng có tỷ lệ thành công thay đổi trong việc loại bỏ các cơn nhịp tim nhanh, từ 13 – 82% và ≤20 % bệnh nhân có thể ngừng điều trị.[323] Xét về tỷ lệ thành công xuất sắc và nguy cơ triệt phá tối thiểu ở các trường hợp có triệu chứng, giá trị điều trị thuốc chống loạn nhịp kéo dài dường như rất hạn chế.
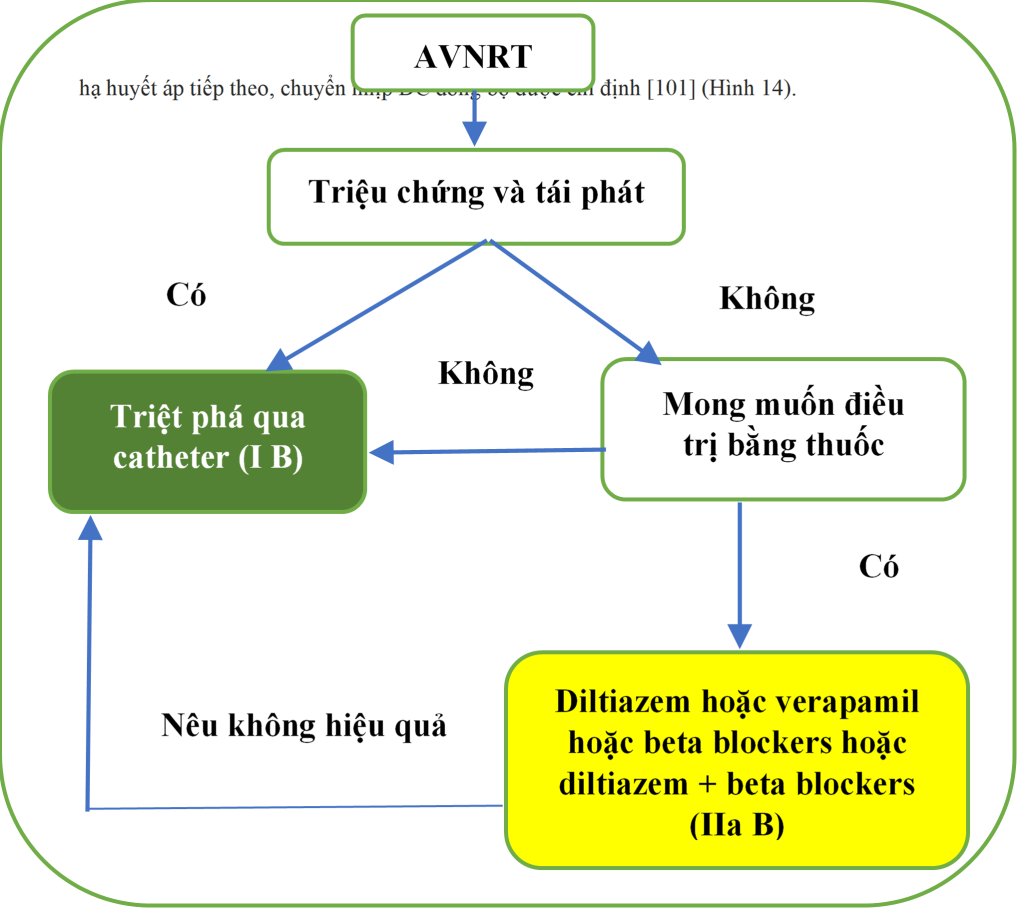
Hình 15. Điều trị lâu dài nhịp nhanh vào lại nút nhĩ thất. AVNRT = nhịp nhanh vào lại nút nhĩ thất.
11.2.2 Nhịp nhanh bộ nối ngoại vị
Nhịp nhanh bộ nối ngoại vị (Junctional ectopic tachycardia: JET), hoặc nhịp nhanh bộ nối ổ, là rối loạn nhịp tim không phổ biến phát sinh do tính tự động bất thường trong AVN hoặc đầu gần của bó His. Nhịp tim nhanh bộ nối ở trẻ em có thể được xem là rối loạn nhịp tim bẩm sinh hoặc, thường xuyên hơn, sớm sau phẫu thuật tim hở ở trẻ sơ sinh. [366.367] Nhịp tim nhanh bẩm sinh có tử suất và bệnh suất đáng kể. Nhịp nhanh cũng có thể được nhận thấy ở những bệnh nhân trưởng thành có tim bình thường về cấu trúc, [369.370] và trong quá khứ có liên quan đến MI cấp tính không tiêu sợi huyết. [371] Phát hiện ECG thông thường trong JET là nhịp nhanh QRS hẹp với khoảng RP ngắn hoặc phân ly AV. Đôi khi, nhịp nhanh có thể không đều và giống với AF.
Propranolol (i.v.) có hoặc không có Procainamide, [370] verapamil, hoặc Procainamide, [372] hoặc flecainide, [373] có thể được sử dụng để điều trị cấp thời, nhưng dữ liệu còn hiếm. Amiodarone (iv) là thuốc được lựa chọn cho JET sau phẫu thuật cũng như để ngăn ngừa JET sớm ở trẻ sau phẫu thuật tim hở. [368,376 – 379] Đối với việc điều trị kéo dài, propranolol [370] hoặc, trong trường hợp không có bệnh tim thiếu máu cục bộ hoặc cấu trúc, flecainide [380] và propafenone, [381] có thể được thử. Triệt phá qua catheter có chọn lọc tại vị trí kích hoạt tâm nhĩ sớm nhất là khả thi, nhưng mang lại tỷ lệ thành công thấp hơn và nguy cơ block AV cao hơn so với AVNRT (5 – 10%). [369,382] Triệt phá bằng nhiệt lạnh (cryo) an toàn hơn. [375,383]
Nhịp nhanh bộ nối không thành cơn (Non-paroxysmal junctional tachycardia) thường đã được chẩn đoán trước đây như là nhịp bộ nối khởi phát và cắt cơn từ từ, với tần số giữa 70–130 b.p.m., và được xem xét mẫu điển hình của DADs được tạo ra do digoxine và được hoạt động khởi kích ở AVN.[3] Khoảng RP trong quá trình nhịp nhân là thay đổi. Thiếu máu cơ tim cục bộ, hạ kali, bệnh phổi tắc nghẽn mạn tính (COPD), và viên cơ tim cũng là những trạng thái kết hợp.
Nhịp nhanh không vào lại tại nút nhĩ thất gây ra do sự dẫn truyền đồng thời nhiều đường nút (thường được gọi là bệnh lý bùng nổ kép hoặc nhịp tim nhanh nút nhĩ thất kép) là một cơ chế không phổ biến của nhịp tim nhanh nút nhĩ thất, [384.385] và được kết hợp với hiện tượng ẩn dẫn ngược lặp lại hoặc “kết nối”.[386-388] Chúng được biểu hiện dưới dạng các khoảng ngưng thất với liên hệ AV cố định sau ngừng, và có thể thường chẩn đoán nhầm như AF. [389] Nhịp nhanh cực kỳ hiếm này có thể gây ra TMC và đáp ứng với triệt phá đường chậm.
(Còn nữa)
Tài liệu tham khảo
- Blomstro¨m-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, Haines DE, Kuck KH, Lerman BB, Miller DD, Shaeffer CW, Stevenson WG, Tomaselli GF. ACC/AHA/ESC guidelines for the management ofpatients with supraventricular arrhythmias–executive summary: a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol 2003;42:14931531.
- Page RL, Joglar JA, Caldwell MA, Calkins H, Conti JB, Deal BJ, Estes NAM, Field ME, Goldberger ZD, Hammill SC, Indik JH, Lindsay BD, Olshansky B, Russo AM, Shen W-K, Tracy CM, Al-Khatib SM. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2016;67:15751623.
- Katritsis DG, Boriani G, Cosio FG, Hindricks G, Jais P, Josephson ME, Keegan R, Kim Y-H, Knight BP, Kuck K-H, Lane DA, Lip GYH, Malmborg H, Oral H, Pappone C, Themistoclakis S, Wood KA, Blomstro¨m-Lundqvist C. European Heart Rhythm Association (EHRA) consensus document on the management of supraventricular arrhythmias, endorsed by Heart Rhythm Society (HRS), AsiaPacific Heart Rhythm Society (APHRS), and Sociedad Latinoamericana de Estimulacion Cardiaca y Electrofisiologia (SOLAECE). Eur Heart J 2018;39:14421445.
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener H-C, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GYH, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37:28932962.
- Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, Badhwar V, Brugada J, Camm J, Chen PS, Chen SA, Chung MK, Nielsen JC, Curtis AB, Davies DW, Day JD, d’Avila A, de Groot N, Di Biase L, Duytschaever M, Edgerton JR, Ellenbogen KA, Ellinor PT, Ernst S, Fenelon G, Gerstenfeld EP, Haines DE, Haissaguerre M, Helm RH, Hylek E, Jackman WM, Jalife J, Kalman JM, Kautzner J, Kottkamp H, Kuck KH, Kumagai K, Lee R, Lewalter T, Lindsay BD, Macle L, Mansour M, Marchlinski FE, Michaud GF, Nakagawa H, Natale A, Nattel S, Okumura K, Packer D, Pokushalov E, Reynolds MR, Sanders P, Scanavacca M, Schilling R, Tondo C, Tsao HM, Verma A, Wilber DJ, Yamane T. 2017 HRS/ EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: executive summary. Europace 2018;20:157208.
- Mairesse GH, Moran P, Van Gelder IC, Elsner C, Rosenqvist M, Mant J, Banerjee A, Gorenek B, Brachmann J, Varma N, Glotz de Lima G, Kalman J, Claes N, Lobban T, Lane D, Lip GYH, Boriani G; ESC Scientific Document Group. Screening for atrial fibrillation: a European Heart Rhythm Association (EHRA) consensus document endorsed by the Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), and Sociedad Latinoamericana de Estimulacion Cardiaca y Electrofisiologia (SOLAECE). Europace 2017;19:15891623.
- Lip GYH, Collet JP, Haude M, Huber K. Management of antithrombotic therapy in AF patients presenting with ACS and/or undergoing PCI: a summary of the Joint Consensus Document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA). Eur Heart J 2018;39:28472850.
- Wit AL, Wellens HJ, Josephson ME. Electrophysiological foundations of cardiac arrhythmias. 1st ed. Minneapolis: Cardiotext Publishing; 2017.
- Orejarena LA, Vidaillet H, DeStefano F, Nordstrom DL, Vierkant RA, Smith PN, Hayes JJ. Paroxysmal supraventricular tachycardia in the general population. J Am Coll Cardiol 1998;31:150157.
- Wu M-H, Chen H-C, Kao F-Y, Huang S-K. Postnatal cumulative incidence of supraventricular tachycardia in a general pediatric population: a national birth cohort database study. Heart Rhythm 2016;13:20702075.
- Garcıa-Fernandez FJ, Ib a~ nez Criado JL, Quesada Dorador A; collaborators of the Spanish Catheter Ablation Registry; REGISTRY COLLABORATORS. Spanish Catheter Ablation Registry. 17th Official Report of the Spanish Society of Cardiology Working Group on Electrophysiology and Arrhythmias (2017). Rev Esp Cardiol (Engl Ed) 2018;71:941951.
- Hosseini SM, Rozen G, Saleh A, Vaid J, Biton Y, Moazzami K, Heist EK, Mansour MC, Kaadan MI, Vangel M, Ruskin JN. Catheter ablation for cardiac arrhythmias: utilization and in-hospital complications, 2000 to 2013. JACC Clin Electrophysiol 2017;3:12401248.
- Holmqvist F, Kesek M, Englund A, Blomstro ¨m-Lundqvist C, Karlsson LO, Kenneb€ack G, Poc¸i D, Samo-Ayou R, Sigurjonsdottir R, Ringborn M, Herczku C, Carlson J, Fengsrud E, Tabrizi F, Ho¨glund N, Lo¨nnerholm S, Kongstad O, Jo¨nsson A, Insulander P. A decade of catheter ablation of cardiac arrhythmias in Sweden: ablation practices and outcomes. Eur Heart J 2019;40:820830.
- Porter MJ, Morton JB, Denman R, Lin AC, Tierney S, Santucci PA, Cai JJ, Madsen N, Wilber DJ. Influence of age and gender on the mechanism of supraventricular tachycardia. Heart Rhythm 2004;1:393396.
- Gonzalez-Torrecilla E, Almendral J, Arenal A, Atienza F, Atea LF, del Castillo S, Fernandez-Aviles F. Combined evaluation of bedside clinical variables and the electrocardiogram for the differential diagnosis of paroxysmal atrioventricular reciprocating tachycardias in patients without pre-excitation. J Am Coll Cardiol 2009;53:23532358.
- Liuba I, Jo¨nsson A, S€afstro¨m K, Walfridsson H. Gender-related differences in patients with atrioventricular nodal reentry tachycardia. Am J Cardiol 2006;97:384388.
- Rosano GMC, Leonardo F, Rosano GMC, De Luca F, Sarrel PM, Beale CM, Collins P. Cyclical variation in paroxysmal supraventricular tachycardia in women. Lancet 1996;347:786788.
- Chang S-H, Kuo C-F, Chou I-J, See L-C, Yu K-H, Luo S-F, Chiou M-J, Zhang W, Doherty M, Wen M-S, Chen W-J, Yeh Y-H. Outcomes associated with paroxysmal supraventricular tachycardia during pregnancy. Circulation 2017;135:616618.
- Krahn AD, Manfreda J, Tate RB, Mathewson FL, Cuddy T. The natural history of electrocardiographic preexcitation in men: the Manitoba Follow-up Study. Ann Intern Med 1992;116:456460.
- Vidaillet HJJ, Pressley JC, Henke E, Harrell FEJ, German LD. Familial occurrence of accessory atrioventricular pathways (preexcitation syndrome). N Engl J Med 1987;317:6569.
- Lu C-W, Wu M-H, Chen H-C, Kao F-Y, Huang S-K. Epidemiological profile of WolffParkinsonWhite syndrome in a general population younger than 50 years of age in an era of radiofrequency catheter ablation. Int J Cardiol 2014;174:530534.
- Skov MW, Rasmussen PV, Ghouse J, Hansen SM, Graff C, Olesen MS, Pietersen A, Torp-Pedersen C, Haunsø S, Køber L, Svendsen JH, Holst AG, Nielsen JB. Electrocardiographic preexcitation and risk of cardiovascular morbidity and mortality. Results from the Copenhagen ECG Study. Circ Arrhythm Electrophysiol 2017;10:e004778.
- Granada J, Uribe W, Chyou P-H, Maassen K, Vierkant R, Smith PN, Hayes J, Eaker E, Vidaillet H. Incidence and predictors of atrial flutter in the general population. J Am Coll Cardiol 2000;36:22422246.
- Withers KL, White J, Carolan-Rees G, Patrick H, O’Callaghan P, Murray S, Cunningham D, Wood KA, Lencioni M, Griffith M. Patient reported outcome measures for cardiac ablation procedures: a multicentre pilot to develop a new questionnaire. Europace 2014;16:16261633.
- Wood KA, Stewart AL, Drew BJ, Scheinman MM, Froelicher ES. Patient perception of symptoms and quality of life following ablation in patients with supraventricular tachycardia. Heart Lung 2010;39:1220.
- White J, Withers KL, Lencioni M, Carolan-Rees G, Wilkes AR, Wood KA, Patrick H, Cunningham D, Griffith M. Cardiff cardiac ablation patient-reported outcome measure (C-CAP): validation of a new questionnaire set for patients undergoing catheter ablation for cardiac arrhythmias in the UK. Qual Life Res 2016;25:15711583.
- Brachmann J, Lewalter T, Kuck KH, Andresen D, Willems S, Spitzer SG, Straube F, Schumacher B, Eckardt L, Danilovic D, Thomas D, Hochadel M, Senges J. Long-term symptom improvement and patient satisfaction following catheter ablation of supraventricular tachycardia: insights from the German ablation registry. Eur Heart J 2017;38:13171326.
- Farkowski MM, Pytkowski M, Maciag A, Golicki D, Wood KA, Kowalik I, Kuteszko R, Szwed H. Gender-related differences in outcomes and resource utilization in patients undergoing radiofrequency ablation of supraventricular tachycardia: results from Patients’ Perspective on Radiofrequency Catheter Ablation of AVRT and AVNRT Study. Europace 2014;16:18211827.
- Feldman A, Voskoboinik A, Kumar S, Spence S, Morton JB, Kistler PM, Sparks PB, Vohra JK, Kalman JM. Predictors of acute and long-term success of slow pathway ablation for atrioventricular nodal reentrant tachycardia: a single center series of 1,419 consecutive patients. Pacing Clin Electrophysiol 2011;34:927933.
- Zimetbaum P, Josephson ME. Evaluation of patients with palpitations. N Engl J Med 1998;338:13691373.
- Page RL, Wilkinson WE, Clair WK, McCarthy EA, Pritchett EL. Asymptomatic arrhythmias in patients with symptomatic paroxysmal atrial fibrillation and paroxysmal supraventricular tachycardia. Circulation 1994;89:224227.
- Thavendiranathan P, Bagai A, Khoo C, Dorian P, Choudhry NK. Does this patient with palpitations have a cardiac arrhythmia? JAMA 2009;302:21352143.
- Leitch JW, Klein GJ, Yee R, Leather RA, Kim YH. Syncope associated with supraventricular tachycardia. An expression of tachycardia rate or vasomotor response? Circulation 1992;85:10641071.
- Thiruganasambandamoorthy V, Rowe BH, Sivilotti MLA, McRae AD, Arcot K, Nemnom MJ, Huang L, Mukarram M, Krahn AD, Wells GA, Taljaard M. Duration of electrocardiographic monitoring of emergency department patients with syncope. Circulation 2019;139:13961406.
- Razavi M, Luria DM, Jahangir A, Hodge DO, Low PA, Shen W-K. Acute blood pressure changes after the onset of atrioventricular nodal reentrant tachycardia: a time-course analysis. J Cardiovasc Electrophysiol 2005;16:10371040.
- Abe H, Nagatomo T, Kobayashi H, Miura Y, Araki M, Kuroiwa A, Nakashima Y. Neurohumoral and hemodynamic mechanisms of diuresis during atrioventricular nodal reentrant tachycardia. Pacing Clin Electrophysiol 1997;20(11):2783-2788.
- Chinen S, Miura M, Tamame T, Matsuoka M, Ohki H, Sumitomo N. Life-threatening atrial tachycardia after the Senning operation in a patient with transposition of the great arteries. Heart Vessels 2012;27:424427.
- Gu ¨rsoy S, Steurer G, Brugada J, Andries E, Brugada P. The hemodynamic mechanism of pounding in the neck in atrioventricular nodal reentrant tachycardia. N Engl J Med 1992;327:772774.
- Contreras-Valdes FM, Josephson ME. IMAGES IN CLINICAL MEDICINE. “Frog sign” in atrioventricular nodal reentrant tachycardia. N Engl J Med 2016;374:e17.
- Lessmeier TJ, Gamperling D, Johnson-Liddon V, Fromm BS, Steinman RT, Meissner MD, Lehmann MH. Unrecognized paroxysmal supraventricular tachycardia: potential for misdiagnosis as panic disorder. Arch Intern Med 1997;157:537543.
- Appelboam A, Reuben A, Mann C, Gagg J, Ewings P, Barton A, Lobban T, Dayer M, Vickery J, Benger J. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet 2015;386:17471753.
- Wang R, Blackburn G, Desai M, Phelan D, Gillinov L, Houghtaling P, Gillinov M. Accuracy of wrist-worn heart rate monitors. JAMA Cardiol 2017;2:104106.
- Katritsis DG, Mark DB, Gersh BJ. Revascularization in stable coronary disease: evidence and uncertainties. Nat Rev Cardiol 2018;15:408419.
- Michowitz Y, Tovia-Brodie O, Heusler I, Sabbag A, Rahkovich M, Shmueli H, Glick A, Belhassen B. Differentiating the QRS morphology of posterior fascicular ventricular tachycardia from right bundle branch block and left anterior hemiblock aberrancy. Circ Arrhythm Electrophysiol 2017;10:e005074.
- Katritsis DG, Josephson ME. Differential diagnosis of regular, narrow-QRS tachycardias. Heart Rhythm 2015;12:16671676.
- Roberts-Thomson KC, Kistler PM, Kalman JM. Focal atrial tachycardia I: clinical features, diagnosis, mechanisms, and anatomic location. Pacing Clin Electrophysiol 2006;29:643652.
- Katritsis DG, Becker A. The atrioventricular nodal reentrant tachycardia circuit: a proposal. Heart Rhythm 2007;4:13541360.
- Jaı ¨s P, Matsuo S, Knecht S, Weerasooriya R, Hocini M, Sacher F, Wright M, Nault I, Lellouche N, Klein G, Cle´menty J, Haı¨ssaguerre M. A deductive mapping strategy for atrial tachycardia following atrial fibrillation ablation: importance of localized reentry. J Cardiovasc Electrophysiol 2009;20:480491. 49. Green M, Heddle B, Dassen W, Wehr M, Abdollah H, Brugada P, Wellens HJ. Value of QRS alteration in determining the site of origin of narrow QRS supraventricular tachycardia. Circulation 1983;68:368373.
- Chen SA, Tai CT, Chiang CE, Chang MS. Role of the surface electrocardiogram in the diagnosis of patients with supraventricular tachycardia. Cardiol Clin 1997;15:539565.
- Morady F. Significance of QRS alternans during narrow QRS tachycardias. Pacing Clin Electrophysiol 1991;14:21932198.
- Crawford TC, Mukerji S, Good E, Chugh A, Bogun F, Pelosi F, Oral H, Morady F, Jongnarangsin K. Utility of atrial and ventricular cycle length variability in determining the mechanism of paroxysmal supraventricular tachycardia. J Cardiovasc Electrophysiol 2007;18:698703.
- Bogossian H, Ninios I, Frommeyer G, Bandorski D, Eckardt L, Lemke B, Zarse M. U wave during supraventricular tachycardia: simulation of a long RP tachycardia and hiding the common type AVNRT. Ann Noninvasive Electrocardiol 2015;20:292295.
- Nagashima K, Watanabe I, Okumura Y, Kaneko Y, Sonoda K, Kogawa R, Sasaki N, Iso K, Takahashi K, Kurokawa S, Nakai T, Ohkubo K, Hirayama A. Ventriculoatrial intervals <_70 ms in orthodromic atrioventricular reciprocating tachycardia. Pacing Clin Electrophysiol 2016;39:11081115.
- Letsas KP, Weber R, Herrera Siklody C, Mihas CC, Stockinger J, Blum T, Kalusche D, Arentz T. Electrocardiographic differentiation of common type atrioventricular nodal reentrant tachycardia from atrioventricular reciprocating tachycardia via a concealed accessory pathway. Acta Cardiologica 2010;65:171176.
- Kalbfleisch SJ, el-Atassi R, Calkins H, Langberg JJ, Morady F. Differentiation of paroxysmal narrow QRS complex tachycardias using the 12-lead electrocardiogram. J Am Coll Cardiol 1993;21:8589.
- Tai CT, Chen SA, Chiang CE, Lee SH, Wen ZC, Chiou CW, Ueng KC, Chen YJ, Yu WC, Chang MS. A new electrocardiographic algorithm using retrograde P waves for differentiating atrioventricular node reentrant tachycardia from atrioventricular reciprocating tachycardia mediated by concealed accessory pathway. J Am Coll Cardiol 1997;29:394402.
- Di Toro D, Hadid C, Lopez C, Fuselli J, Luis V, Labadet C. Utility of the aVL lead in the electrocardiographic diagnosis of atrioventricular node re-entrant tachycardia. Europace 2009;11:944948.
- Haghjoo M, Bahramali E, Sharifkazemi M, Shahrzad S, Peighambari M. Value of the aVR lead in differential diagnosis of atrioventricular nodal reentrant tachycardia. Europace 2012;14:16241628.
- Knight BP, Ebinger M, Oral H, Kim MH, Sticherling C, Pelosi F, Michaud GF, Strickberger SA, Morady F. Diagnostic value of tachycardia features and pacing maneuvers during paroxysmal supraventricular tachycardia. J Am Coll Cardiol 2000;36:574582.
- Markowitz SM, Stein KM, Mittal S, Slotwtner DJ, Lerman BB. Differential effects of adenosine on focal and macroreentrant atrial tachycardia. J Cardiovasc Electrophysiol 1999;10:489502.
- Alzand BSN, Manusama R, Gorgels APM, Wellens HJJ. An “almost wide” QRS tachycardia. Circ Arrhythm Electrophysiol 2009;2:e1e3.
- Alzand BSN, Crijns HJ. Diagnostic criteria of broad QRS complex tachycardia: decades of evolution. Europace 2011;13:465472.
- Stewart RB, Bardy GH, Greene H. Wide complex tachycardia: misdiagnosis and outcome after emergent therapy. Ann Intern Med 1986;104:766771.
- Wellens HJJ. Ventricular tachycardia: diagnosis of broad QRS complex tachycardia. Heart 2001;86:579585.
- Willems S, Shenasa M, Borggrefe M, Hindricks G, Chen X, Rotman B, Kottkamp H, Haverkamp W, Breithardt G. Atrioventricular nodal reentry tachycardia: electrophysiologic comparisons in patients with and without 2:1 infra-His block. Clin Cardiol 1993;16:883888.
- Ranger S, Talajic M, Lemery R, Roy D, Villemaire C, Nattel S. Kinetics of usedependent ventricular conduction slowing by antiarrhythmic drugs in humans. Circulation 1991;83:19871994.
- Jastrzebski M, Kukla P, Czarnecka D, Kawecka-Jaszcz K. Comparison of five electrocardiographic methods for differentiation of wide QRS-complex tachycardias. Europace 2012;14:11651171.
- Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation 1991;83:16491659.
- Kindwall KE, Brown J, Josephson ME. Electrocardiographic criteria for ventricular tachycardia in wide complex left bundle branch block morphology tachycardias. Am J Cardiol 1988;61:12791283.
- Vereckei A, Duray G, Sze´nasi G, Altemose GT, Miller JM. New algorithm using only lead aVR for differential diagnosis of wide QRS complex tachycardia. Heart Rhythm 2008;5:8998.
- Pava LF, Perafan P, Badiel M, Arango JJ, Mont L, Morillo CA, Brugada J. R-wave peak time at DII: a new criterion for differentiating between wide complex QRS tachycardias. Heart Rhythm 2010;7:922926.
- Steurer G, Gursoy S, Frey B, Simonis F, Andries E, Kuck K, Brugada P. The differential diagnosis on the electrocardiogram between ventricular tachycardia and preexcited tachycardia. Clin Cardiol 1994;17:306308.
- Jastrzebski M, Moskal P, Kukla P, Fijorek K, Kisiel R, Czarnecka D. Specificity of wide QRS complex tachycardia criteria and algorithms in patients with ventricular preexcitation. Ann Noninvasive Electrocardiol 2018;23:e12493.
- Alberca T, Almendral J, Sanz P, Almazan A, Cantalapiedra JL, Delcan JL. Evaluation of the specificity of morphological electrocardiographic criteria for the differential diagnosis of wide QRS complex tachycardia in patients with intraventricular conduction defects. Circulation 1997;96:35273533.
- Ceresnak SR, Liberman L, Avasarala K, Tanel R, Motonaga KS, Dubin AM. Are wide complex tachycardia algorithms applicable in children and patients with congenital heart disease? J Electrocardiol 2010;43:694700.
- Jastrzebski M, Kukla P, Czarnecka D, Kawecka-Jaszcz K. Specificity of the wide QRS complex tachycardia algorithms in recipients of cardiac resynchronization therapy. J Electrocardiol 2012;45:319326.
- Lau EW, Ng GA. Comparison of the performance of three diagnostic algorithms for regular broad complex tachycardia in practical application. Pacing Clin Electrophysiol 2002;25:822827.
- Isenhour JL, Craig S, Gibbs M, Littmann L, Rose G, Risch R. Wide-complex tachycardia: continued evaluation of diagnostic criteria. Acad Emerg Med 2000;7:769773.
- Baxi RP, Hart KW, Vereckei A, Miller J, Chung S, Chang W, Gottesman B, Hunt M, Culyer G, Trimarco T, Willoughby C, Suarez G, Lindsell CJ, Collins SP. Vereckei criteria as a diagnostic tool amongst emergency medicine residents to distinguish between ventricular tachycardia and supra-ventricular tachycardia with aberrancy. J Cardiol 2012;59:307312.
- Jastrzebski M, Sasaki K, Kukla P, Fijorek K, Stec S, Czarnecka D. The ventricular tachycardia score: a novel approach to electrocardiographic diagnosis of ventricular tachycardia. Europace 2016;18:578584.
- Yadav AV, Nazer B, Drew BJ, Miller JM, El Masry H, Groh WJ, Natale A, Marrouche N, Badhwar N, Yang Y, Scheinman MM. Utility of conventional electrocardiographic criteria in patients with idiopathic ventricular tachycardia. JACC Clin Electrophysiol 2017;3:669677.
- Knight BP, Zivin A, Souza J, Goyal R, Man KC, Strickberger A, Morady F. Use of adenosine in patients hospitalized in a university medical center. Am J Med 1998;105:275280.
- Jolobe OMP. Caveats in preexcitation-related atrial fibrillation. Am J Emerg Med 2010;28:252253.
- Murman DH, McDonald AJ, Pelletier AJ, Camargo CA. U.S. Emergency Department Visits for Supraventricular Tachycardia, 19932003. Acad Emerg Med 2007;14(6):578-581.
- Roth A, Elkayam I, Shapira I, Sander J, Malov N, Kehati M, Golovner M. Effectiveness of prehospital synchronous direct-current cardioversion for supraventricular tachyarrhythmias causing unstable hemodynamic states. Am J Cardiol 2003;91:489491.
- Wittwer MR, Rajendran S, Kealley J, Arstall MA. A South Australian registry of biphasic cardioversions of atrial arrhythmias: efficacy and predictors of success. Heart Lung Circ 2015;24:342347.
- Reisinger J, Gstrein C, Winter T, Zeindlhofer E, Ho¨llinger K, Mori M, Schiller A, Winter A, Geiger H, Siostrzonek P. Optimization of initial energy for cardioversion of atrial tachyarrhythmias with biphasic shocks. Am J Emerg Med 2010;28:159165.
- Smith GD, Fry MM, Taylor D, Morgans A, Cantwell K. Effectiveness of the Valsalva Manoeuvre for reversion of supraventricular tachycardia. Cochrane Database Syst Rev 2015;2:CD009502.
- Lim SH, Anantharaman V, Teo WS, Goh PP, Tan ATH. Comparison of treatment of supraventricular tachycardia by Valsalva maneuver and carotid sinus massage. Ann Emerg Med 1998;31:3035.
- Smith G, Morgans A, Boyle M. Use of the Valsalva manoeuvre in the prehospital setting: a review of the literature. Emerg Med J 2009;26:810.
- Brady WJJ, DeBehnke DJ, Wickman LL, Lindbeck G. Treatment of out-of-hospital supraventricular tachycardia: adenosine vs verapamil. Acad Emerg Med 1996;3(6):574-585.
- Glatter KA, Cheng J, Dorostkar P, Modin G, Talwar S, Al-Nimri M, Lee RJ, Saxon LA, Lesh MD, Scheinman MM. Electrophysiologic effects of adenosine in patients with supraventricular tachycardia. Circulation 1999;99:10341040.
- Delaney B, Loy J, Kelly A-M. The relative efficacy of adenosine versus verapamil for the treatment of stable paroxysmal supraventricular tachycardia in adults: a meta-analysis. Eur J Emerg Med 2011;18:148152.
- Dougherty AH, Jackman WM, Naccarelli GV, Friday KJ, Dias VC. Acute conversion of paroxysmal supraventricular tachycardia with intravenous diltiazem. Am J Cardiol 1992;70:587592.
- Hood MA, Smith WM. Adenosine versus verapamil in the treatment of supraventricular tachycardia: A randomized double-crossover trial. Am Heart J 1992;123:15431549.
- Gupta A, Naik A, Vora A, Lokhandwala Y. Comparison of efficacy of intravenous diltiazem and esmolol in terminating supraventricular tachycardia. J Assoc Physicians India 1999;47:969972.
- Lim SH, Anantharaman V, Teo WS, Chan YH. Slow infusion of calcium channel blockers compared with intravenous adenosine in the emergency treatment of supraventricular tachycardia. Resuscitation 2009;80:523528.
- Das G, Tschida V, Gray R, Dhurandhar R, Lester R, McGrew F, Askenazi J, Kaplan K, Emanuele M, Turlapaty P, Hua TA, Hoff J, Allin D, Laddu A. Efficacy of esmolol in the treatment and transfer of patients with supraventricular tachyarrhythmias to alternate oral antiarrhythmic agents. J Clin Pharmacol1988;28:746750.
- Amsterdam EA, Kulcyski J, Ridgeway MG. Efficacy of cardioselective beta-adrenergic blockade with intravenously administered metoprolol in the treatment of supraventricular tachyarrhythmias. J Clin Pharmacol 1991;31:714718.
- Smith G, Taylor DM, Morgans A, Cameron P. Prehospital synchronized electrical cardioversion of a poorly perfused SVT patient by paramedics. Prehosp Disaster Med 2013;28:301304. 102. Wen Z-C, Chen S-A, Tai C-T, Chiang C-E, Chiou C-W, Chang M-S. Electrophysiological mechanisms and determinants of vagal maneuvers for termination of paroxysmal supraventricular tachycardia. Circulation 1998;98:27162723.
- Taylor DM, Wong LF. Incorrect instruction in the use of the Valsalva manoeuvre for paroxysmal supra-ventricular tachycardia is common. Emergency Medicine 2004;16(4):284-287.
- Smith G, Boyle MJ. The 10 mL syringe is useful in generating the recommended standard of 40 mmHg intrathoracic pressure for the Valsalva manoeuvre. Emerg Med Australas 2009;21:449454.
- Layland J, Carrick D, Lee M, Oldroyd K, Berry C. Adenosine: physiology, pharmacology, and clinical applications. JACC Cardiovasc Interv 2014;7:581591.
- Lerman BB, Markowitz SM, Cheung JW, Liu CF, Thomas G, Ip JE. Supraventricular tachycardia. Circ Arrhythm Electrophysiol 2018;11:e006953.
- Camm AJ, Garratt CJ. Adenosine and supraventricular tachycardia. N Engl J Med 1991;325:16211629.
- Ng GA, Martin W, Rankin AC. Imaging of adenosine bolus transit following intravenous administration: insights into antiarrhythmic efficacy. Heart 1999;82:163169.
- Alabed S, Sabouni A, Providencia R, Atallah E, Qintar M, Chico TJA. Adenosine versus intravenous calcium channel antagonists for supraventricular tachycardia. Cochrane Database Syst Rev 2017;10:CD005154.
- Cabalag MS, Taylor DM, Knott JC, Buntine P, Smit D, Meyer A. Recent caffeine ingestion reduces adenosine efficacy in the treatment of paroxysmal supraventricular tachycardia. Acad Emerg Med 2010;17:4449.
- Karydes HC, Bryant SM. Adenosine and caffeine-induced paroxysmal supraventricular tachycardia. Acad Emerg Med 2010;17:570570. 112. Burki NK, Wheeler JD, Lu-Yuan L. Intravenous adenosine and dyspnea in humans. J Appl Physiol (1985) 2005;98:180185.
- Fragakis N, Antoniadis AP, Korantzopoulos P, Kyriakou P, Koskinas KC, Geleris P. Sinus nodal response to adenosine relates to the severity of sinus node dysfunction. Europace 2012;14:859864.
- Ellenbogen KA, Thames MD, DiMarco JP, Sheehan H, Lerman BB. Electrophysiological effects of adenosine in the transplanted human heart. Evidence of supersensitivity. Circulation 1990;81:821828.
- Toft J, Mortensen J, Hesse B. Risk of atrioventricular block during adenosine pharmacologic stress testing in heart transplant recipients. Am J Cardiol 1998;82:696697.
- Flyer JN, Zuckerman WA, Richmond ME, Anderson BR, Mendelsberg TG, McAllister JM, Liberman L, Addonizio LJ, Silver ES. Prospective study of adenosine on atrioventricular nodal conduction in pediatric and young adult patients after heart transplantation. Circulation 2017;135:24852493.
- Ip JE, Cheung JW, Chung JH, Liu CF, Thomas G, Markowitz SM, Lerman BB. Adenosine-induced atrial fibrillation. Insights into mechanism. Circ Arrhythm Electrophysiol 2013;6:e34e37.
- Li N, Csepe TA, Hansen BJ, Sul LV, Kalyanasundaram A, Zakharkin SO, Zhao J, Guha A, Van Wagoner DR, Kilic A, Mohler PJ, Janssen PML, Biesiadecki BJ, Hummel JD, Weiss R, Fedorov VV. adenosine-induced atrial fibrillation. Localized reentrant drivers in lateral right atria due to heterogeneous expression of adenosine A1 receptors and GIRK4 subunits in the human heart. Circulation 2016;134:486498.
- Turley AJ, Murray S, Thambyrajah J. Pre-excited atrial fibrillation triggered by intravenous adenosine: a commonly used drug with potentially life-threatening adverse effects. Emerg Med J 2008;25:4648.
- Garratt CJ, Griffith MJ, O’Nunain S, Ward DE, Camm AJ. Effects of intravenous adenosine on antegrade refractoriness of accessory atrioventricular connections. Circulation 1991;84:19621968.
- Coli S, Mantovani F, Ferro J, Gonzi G, Zardini M, Ardissino D. Adenosineinduced severe bronchospasm in a patient without pulmonary disease. Am J Emerg Med 2012;30:2082.e32082.e5.
- Cerqueira MD, Verani MS, Schwaiger M, Heo J, Iskandrian AS. Safety profile of adenosine stress perfusion imaging: results from the adenoscan multicenter trial registry. J Am Coll Cardiol 1994;23:384389.
- Balan KK, Critchley M. Is the dyspnea during adenosine cardiac stress test caused by bronchospasm? Am Heart J 2001;142:142145.
- Cushley MJ, Tattersfield AE, Holgate ST. Inhaled adenosine and guanosine on airway resistance in normal and asthmatic subjects. Br J Clin Pharmacol 2004;58:S751S755.
- Burki NK, Alam M, Lee L-Y. The pulmonary effects of intravenous adenosine in asthmatic subjects. Respiratory Research 2006;7:139139.
- Burkhart KK. Respiratory failure following adenosine administration. Am J Emerg Med 1993;11:249250.
- DeGroff CG, Silka MJ. Bronchospasm after intravenous administration of adenosine in a patient with asthma. J Pediatr 1994;125:822823.
- Brubaker S, Long B, Koyfman A. Alternative treatment options for atrioventricular-nodal-reentry tachycardia: an emergency medicine review. J Emerg Med 2018;54:198206.
- Stambler BS, Dorian P, Sager PT, Wight D, Douville P, Potvin D, Shamszad P, Haberman RJ, Kuk RS, Lakkireddy DR, Teixeira JM, Bilchick KC, Damle RS, Bernstein RC, Lam WW, O’Neill G, Noseworthy PA, Venkatachalam KL, Coutu B, Mondesert B, Plat F. Etripamil nasal spray for rapid conversion of supraventricular tachycardia to sinus rhythm. J Am Coll Cardiol2018;72:489497.
- Olasveengen TM, de Caen AR, Mancini ME, Maconochie IK, Aickin R, Atkins DL, Berg RA, Bingham RM, Brooks SC, Castre´n M, Chung SP, Considine J, Couto TB, Escalante R, Gazmuri RJ, Guerguerian AM, Hatanaka T, Koster RW, Kudenchuk PJ, Lang E, Lim SH, Løfgren B, Meaney PA, Montgomery WH Morley PT, Morrison LJ, Nation KJ, Ng KC, Nadkarni VM, Nishiyama C, Nuthall G, Ong GY, Perkins GD, Reis AG, Ristagno G, Sakamoto T, Sayre MR, Schexnayder SM, Sierra AF, Singletary EM, Shimizu N, Smyth MA, Stanton D, Tijssen JA, Travers A, Vaillancourt C, Van de Voorde P, Hazinski MF, Nolan JP; ILCOR Collaborators. 2017 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations summary. Circulation 2017;136:e424e440.
- Priori SG, Blomstro¨m-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekva˚l TM, Spaulding C, Van Veldhuisen DJ, Kolh P, Lip GYH, Agewall S, Baron-Esquivias G, Boriani G, Budts W, Bueno H, Capodanno D, Carerj S, Crespo-Leiro MG, Czerny M, Deaton C, Dobrev D, Erol C¸, Galderisi M, Gorenek B, Kriebel T, Lambiase P, Lancellotti P, Lane DA, Lang I, Manolis AJ, Morais J, Moreno J, Piepoli MF, Rutten FH, Sredniawa B, Zamorano JL, Zannad F. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC) Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36:27932867.
- Ortiz M, Martin A, Arribas F, Coll-Vinent B, Del Arco C, Peinado R, Almendral J; PROCAMIO Study Investigators. Randomized comparison of intravenous procainamide vs. intravenous amiodarone for the acute treatment of tolerated wide QRS tachycardia: the PROCAMIO study. Eur Heart J 2017;38:13291335.
- Buxton AE, Marchlinski FE, Doherty JU, Flores B, Josephson ME. Hazards of intravenous verapamil for sustained ventricular tachycardia. Am J Cardiol 1987;59:11071110.
- Dancy M, Camm AJ, Ward D. Misdiagnosis of chronic recurrent ventricular tachycardia. Lancet 1985;326:320323.
- Crijns HJ, Lie KI. Haemodynamic deterioration after treatment with adenosine. Br Heart J 1995;73:103.
- Gorgels APM, van den Dool A, Hofs A, Mulleneers R, Smeets JLRM, Vos MA, Wellens HJJ. Comparison of procainamide and lidocaine in terminating sustained monomorphic ventricular tachycardia. Am J Cardiol 1996;78:4346.
- Scheinman MM, Levine JH, Cannom DS, Friehling T, Kopelman HA, Chilson DA, Platia EV, Wilber DJ, Kowey PR. Dose-ranging study of intravenous amiodarone in patients with life-threatening ventricular tachyarrhythmias. Circulation 1995;92:32643272.
- Levine JH, Massumi A, Scheinman MM, Winkle RA, Platia EV, Chilson DA, Gomes JA, Woosley RL. Intravenous amiodarone for recurrent sustained hypotensive ventricular tachyarrhythmias. J Am Coll Cardiol 1996;27:6775.
- Olshansky B, Sullivan RM. Inappropriate sinus tachycardia. Europace 2019;21:194207.
- Still A-M, Raatikainen P, Ylitalo A, Kauma H, Ik€aheimo M, Kes€aniemi YA, Huikuri HV. Prevalence, characteristics and natural course of inappropriate sinus tachycardia. Europace 2005;7:104112.
- Baruscotti M, Bucchi A, Milanesi R, Paina M, Barbuti A, Gnecchi-Ruscone T, Bianco E, Vitali-Serdoz L, Cappato R, DiFrancesco D. A gain-of-function mutation in the cardiac pacemaker HCN4 channel increasing cAMP sensitivity is associated with familial Inappropriate Sinus Tachycardia. Eur Heart J 2017;38:280288.
- Ruzieh M, Moustafa A, Sabbagh E, Karim MM, Karim S. Challenges in treatment of inappropriate sinus tachycardia. Curr Cardiol Rev 2018;14:4244.
- Brunner S, Herbel R, Drobesch C, Peters A, Massberg S, Kaab S, Sinner MF. Alcohol consumption, sinus tachycardia, and cardiac arrhythmias at the Munich Octoberfest: results from the Munich Beer Related Electrocardiogram Workup Study (MunichBREW). Eur Heart J 2017;38:21002106.
- Shen WK. How to manage patients with inappropriate sinus tachycardia. Heart Rhythm 2005;2:10151019.
- Foster MC, Levine PA. Use of verapamil to control an inappropriate chronic sinus tachycardia. Chest 1984;85:697699.
- Cappato R, Castelvecchio S, Ricci C, Bianco E, Vitali-Serdoz L, GnecchiRuscone T, Pittalis M, De Ambroggi L, Baruscotti M, Gaeta M, Furlanello F, Di Francesco D, Lupo PP. Clinical efficacy of ivabradine in patients with inappropriate sinus tachycardia: a prospective, randomized, placebo-controlled, doubleblind, crossover evaluation. J Am Coll Cardiol 2012;60:13231329.
- Ptaszynski P, Kaczmarek K, Ruta J, Klingenheben T, Wranicz JK. Metoprolol succinate vs. ivabradine in the treatment of inappropriate sinus tachycardia in patients unresponsive to previous pharmacological therapy. Europace 2013;15:116121.
- Benezet-Mazuecos J, Rubio JM, FarrE J, Qui~NOnes MA, Sanchez-Borque P, MacIA E. Long-term outcomes of ivabradine in inappropriate sinus tachycardia patients: appropriate efficacy or inappropriate patients. Pacing Clin Electrophysiol 2013;36:830836.
- Cal o L, Rebecchi M, Sette A, Martino A, de Ruvo E, Sciarra L, De Luca L, Zuccaro LM, Giunta G, Ciccaglioni A, Lioy E, Fedele F. Efficacy of ivabradine administration in patients affected by inappropriate sinus tachycardia. Heart Rhythm 2010;7:13181323.
- Ptaszynski P, Kaczmarek K, Ruta J, Klingenheben T, Wranicz JK. Ivabradine in the treatment of inappropriate sinus tachycardia in patients after successful radiofrequency catheter ablation of atrioventricular node slow pathway. Pacing Clin Electrophysiol 2013;36:4249.
- Dias da Silva VJ, Tobaldini E, Rocchetti M, Wu MA, Malfatto G, Montano N, Zaza A. Modulation of sympathetic activity and heart rate variability by ivabradine. Cardiovasc Res 2015;108:3138.
- Ptaszynski P, Kaczmarek K, Ruta J, Klingenheben T, Cygankiewicz I, Wranicz JK. Ivabradine in combination with metoprolol succinate in the treatment of inappropriate sinus tachycardia. J Cardiovasc Pharmacol Ther 2013;18:338344.
- Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, Blomstro¨m-Lundqvist C, Cıfkova R, De Bonis M, Iung B, Johnson MR, Kintscher U, Kranke P, Lang IM, Morais J, Pieper PG, Presbitero P, Price S, Rosano GMC, Seeland U, Simoncini T, Swan L, Warnes CA; ESC Scientific Document Group. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J 2018:39:31653241.
- Yu J, Zhou Z, Tay-Sontheimer J, Levy RH, Ragueneau-Majlessi I. Risk of clinically relevant pharmacokinetic-based drug-drug interactions with drugs approved by the U.S. Food and Drug Administration between 2013 and 2016. Drug Metab Dispos 2018;46:835845.
- Man KC, Knight B, Tse H-F, Pelosi F, Michaud GF, Flemming M, Strickberger SA, Morady F. Radiofrequency catheter ablation of inappropriate sinus tachycardia guided by activation mapping. J Am Coll Cardiol 2000;35:451457.
- Marrouche NF, Beheiry S, Tomassoni G, Cole C, Bash D, Dresing T, Saliba W, Abdul-Karim A, Tchou P, Schweikert R, Leonelli F, Natale A. Three-dimensional nonfluoroscopic mapping and ablation of inappropriate sinus tachycardia: procedural strategies and long-term outcome. J Am Coll Cardiol 2002;39:10461054.
- Callans DJ, Ren J-F, Schwartzman D, Gottlieb CD, Chaudhry FA, Marchlinski FE. Narrowing of the superior vena cavaright atrium junction during radiofrequency catheter ablation for inappropriate sinus tachycardia: analysis with intracardiac echocardiography. J Am Coll Cardiol 1999;33:16671670.
- Takemoto M, Mukai Y, Inoue S, Matoba T, Nishizaka M, Ide T, Chishaki A, Sunagawa K. Usefulness of non-contact mapping for radiofrequency catheter ablation of inappropriate sinus tachycardia: new procedural strategy and longterm clinical outcome. Intern Med 2012;51:357362.
- Koplan BA, Parkash R, Couper G, Stevenson WG. Combined epicardial-endocardial approach to ablation of inappropriate sinus tachycardia. J Cardiovasc Electrophysiol 2004;15:237240.
- Jacobson JT, Kraus A, Lee R, Goldberger JJ. Epicardial/endocardial sinus node ablation after failed endocardial ablation for the treatment of inappropriate sinus tachycardia. J Cardiovasc Electrophysiol 2014;25:236241.
- Rodr ıguez-Ma~nero M, Kreidieh B, Al Rifai M, Ibarra-Cortez S, Schurmann P, Alvarez PA, Fernandez-Lopez XA, Garcıa-Seara J, Martınez-Sande L, GonzalezJuanatey JR, Valderrabano M. Ablation of inappropriate sinus tachycardia: a systematic review of the literature. JACC Clin Electrophysiol 2017;3:253265.
- Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system. N Engl J Med 2001;344:501509.
- Gomes JA, Hariman RJ, Kang PS, Chowdry IH. Sustained symptomatic sinus node reentrant tachycardia: Incidence, clinical significance, electrophysiologic observations and the effects of antiarrhythmic agents. J Am Coll Cardiol 1985;5:4557.
- Malik AK, Ching CK, Liew R, Chong DT, Teo WS. Successful ablation of sinus node reentrant tachycardia using remote magnetic navigation system. Europace 2012;14:455456.
- Cossu SF, Steinberg JS. Supraventricular tachyarrhythmias involving the sinus node: clinical and electrophysiologic characteristics. Prog Cardiovasc Dis 1998;41:5163.
- Sanders WE Jr, Sorrentino RA, Greenfield RA, Shenasa H, Hamer ME, Wharton JM. Catheter ablation of sinoatrial node reentrant tachycardia. J Am Coll Cardiol 1994;23:926934.
- Fu Q, VanGundy TB, Shibata S, Auchus RJ, Williams GH, Levine BD. Exercise training versus propranolol in the treatment of the postural orthostatic tachycardia syndrome. Hypertension 2011;58:167175.
- Fu Q, VanGundy TB, Galbreath MM, Shibata S, Jain M, Hastings JL, Bhella PS, Levine BD. Cardiac origins of the postural orthostatic tachycardia syndrome. J Am Coll Cardiol 2010;55:28582868.
- Winker R, Barth A, Bidmon D, Ponocny I, Weber M, Mayr O, Robertson D, Diedrich A, Maier R, Pilger A, Haber P, Ru¨diger HW. Endurance exercise training in orthostatic intolerance. A randomized, controlled trial 2005;45: 391398.
- Jacob G, Shannon JR, Black B, Biaggioni I, Mosqueda-Garcia R, Robertson RM, Robertson D. Effects of volume loading and pressor agents in idiopathic orthostatic tachycardia. Circulation 1997;96:575580.
- Raj SR, Biaggioni I, Yamhure PC, Black BK, Paranjape SY, Byrne DW, Robertson D. Renin-aldosterone paradox and perturbed blood volume regulation underlying postural tachycardia syndrome. Circulation 2005;111:15741582.
- Raj SR, Black BK, Biaggioni I, Paranjape SY, Ramirez M, Dupont WD, Robertson D. Propranolol decreases tachycardia and improves symptoms in the postural tachycardia syndrome. Less is more. Circulation 2009;120:725734.
- Kanjwal K, Karabin B, Sheikh M, Elmer L, Kanjwal Y, Saeed B, Grubb BP. Pyridostigmine in the treatment of postural orthostatic tachycardia: A singlecenter experience. Pacing Clin Electrophysiol 2011;34:750755.
- Raj SR, Black BK, Biaggioni I, Harris PA, Robertson D. Acetylcholinesterase inhibition improves tachycardia in postural tachycardia syndrome. Circulation 2005;111:27342740.
- McDonald C, Frith J, Newton JL. Single centre experience of ivabradine in postural orthostatic tachycardia syndrome. Europace 2011;13:427430.
- Glukhov AV, Hage LT, Hansen BJ, Pedraza-Toscano A, Vargas-Pinto P, Hamlin RL, Weiss R, Carnes CA, Billman GE, Fedorov VV. Sinoatrial node reentry in a canine chronic left ventricular infarct model: role of intranodal fibrosis and heterogeneity of refractoriness. Circ Arrhythm Electrophysiol 2013;6:984994.
- Sheldon RS, Grubb BP, Olshansky B, Shen W-K, Calkins H, Brignole M, Raj SR, Krahn AD, Morillo CA, Stewart JM, Sutton R, Sandroni P, Friday KJ, Hachul DT, Cohen MI, Lau DH, Mayuga KA, Moak JP, Sandhu RK, Kanjwal K. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm 2015;12:e41e63.
- Bryarly M, Phillips LT, Fu Q, Vernino S, Levine BD. Postural orthostatic tachycardia syndrome: JACC Focus Seminar. J Am Coll Cardiol 2019;73:12071228.
- Benarroch EE. Postural tachycardia syndrome: a heterogeneous and multifactorial disorder. Mayo Clinic Proceedings 2012;87:12141225.
- Tomichi Y, Kawano H, Mukaino A, Chiba A, Doi Y, Arakawa S, Ishimatsu T, Fukae S, Abiru N, Maemura K. Postural orthostatic tachycardia in a patient with type 2 diabetes with diabetic neuropathy. Int Heart J 2018;59:14881490.
- Low PA, Sandroni P, Joyner M, Shen WK. Postural tachycardia syndrome (POTS). J Cardiovasc Electrophysiol 2009;20:352358.
- Fedorowski A. Postural orthostatic tachycardia syndrome: clinical presentation, aetiology, and management. J Intern Med 2018;285:352366.
- Poutiainen AM, Koistinen MJ, Airaksinen KE, Hartikainen EK, Kettunen RVJ, Karjalainen JE, Huikuri HV. Prevalence and natural course of ectopic atrial tachycardia. Eur Heart J 1999;20:694700.
- Kistler PM, Sanders P, Fynn SP, Stevenson IH, Hussin A, Vohra JK, Sparks PB, Kalman JM. Electrophysiological and electrocardiographic characteristics of focal atrial tachycardia originating from the pulmonary veins: acute and long-term outcomes of radiofrequency ablation. Circulation 2003;108:19681975.
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659666.
- Kistler PM, Roberts-Thomson KC, Haqqani HM, Fynn SP, Singarayar S, Vohra JK, Morton JB, Sparks PB, Kalman JM. P-wave morphology in focal atrial tachycardia: development of an algorithm to predict the anatomic site of origin. J Am Coll Cardiol 2006;48:10101017.
- Chen SA, Chiang CE, Yang CJ, Cheng CC, Wu TJ, Wang SP, Chiang BN, Chang MS. Sustained atrial tachycardia in adult patients. Electrophysiological characteristics, pharmacological response, possible mechanisms, and effects of radiofrequency ablation. Circulation 1994;90:12621278.
- Mehta AV, Sanchez GR, Sacks EJ, Casta A, Dunn JM, Donner RM. Ectopic automatic atrial tachycardia in children: clinical characteristics, management and follow-up. J Am Coll Cardiol 1988;11:379385.
- Hohnloser SH, Zabel M. Short- and long-term efficacy and safety of flecainide acetate for supraventricular arrhythmias. Am J Cardiol 1992;70:A3A10.
- Kunze K-P, Kuck K-H, Schlu¨ter M, Bleifeld W. Effect of encainide and flecainide on chronic ectopic atrial tachycardia. J Am Coll Cardiol 1986;7:11211126.
- Eidher U, Freihoff F, Kaltenbrunner W, Steinbach K. Efficacy and safety of ibutilide for the conversion of monomorphic atrial tachycardia. Pacing Clin Electrophysiol 2006;29:358362.
- Vietti-Ramus G, Veglio F, Marchisio U, Burzio P, Latini R. Efficacy and safety of short intravenous amiodarone in supraventricular tachyarrhythmias. Int J Cardiol 1992;35:7785.
- Salem JE, Dureau P, Funck-Brentano C, Hulot JS, El-Aissaoui M, Aissaoui N, Urien S, Faisy C. Effectiveness of heart rate control on hemodynamics in critically ill patients with atrial tachyarrhythmias managed by amiodarone. Pharmacol Res 2017;122:118126.
- Anguera I, Brugada J, Roba M, Mont Ls, Aguinaga L, Geelen P, Brugada P. Outcomes after radiofrequency catheter ablation of atrial tachycardia. Am J Cardiol 2001;87:886890.
- Biviano AB, Bain W, Whang W, Leitner J, Dizon J, Hickey K, Garan H. Focal left atrial tachycardias not associated with prior catheter ablation for atrial fibrillation: clinical and electrophysiological characteristics. Pacing Clin Electrophysiol 2012;35:1727.
- Medi C, Kalman JM, Haqqani H, Vohra JK, Morton JB, Sparks PB, Kistler PM. Tachycardia-mediated cardiomyopathy secondary to focal atrial tachycardia: long-term outcome after catheter ablation. J Am Coll Cardiol 2009;53:17911797.
- Ouyang F, Ma J, Ho SY, B€ansch D, Schmidt B, Ernst S, Kuck K-H, Liu S, Huang H, Chen M, Chun J, Xia Y, Satomi K, Chu H, Zhang S, Antz M. Focal atrial tachycardia originating from the non-coronary aortic sinus: electrophysiological characteristics and catheter ablation. J Am Coll Cardiol 2006;48:122131.
- Heusch A, Kramer HH, Krogmann ON, Rammos S, Bourgeois M. Clinical experience with propafenone for cardiac arrhythmias in the young. Eur Heart J 1994;15:10501056.
- Meles E, Carbone C, Maggiolini S, Moretti P, CC DECGentile G, GnecchiRuscone T. A case of atrial tachycardia treated with ivabradine as bridge to ablation. J Cardiovasc Electrophysiol 2015;26:565568.
- Bohora S, Lokhandwala Y, Parekh P, Vasavda A. Reversal of tachycardiomyopathy due to left atrial tachycardia by ivabradine. J Cardiovasc Electrophysiol 2011;22:340342.
- Guccione P, Paul T, Garson A Jr. Long-term follow-up of amiodarone therapy in the young: continued efficacy, unimpaired growth, moderate side effects. J Am Coll Cardiol 1990;15:11181124.
- von Bernuth G, Engelhardt W, Kramer HH, Singer H, Schneider P, Ulmer H, Brodherr-Heberlein S, Kienast W, Lang D, Lindinger A, Schmidt K. Atrial automatic tachycardia in infancy and childhood. Eur Heart J 1992;13:14101415.
- Spector P, Reynolds MR, Calkins H, Sondhi M, Xu Y, Martin A, Williams CJ, Sledge I. Meta-analysis of ablation of atrial flutter and supraventricular tachycardia. Am J Cardiol 2009;104:671677.
- Bohnen M, Stevenson WG, Tedrow UB, Michaud GF, John RM, Epstein LM, Albert CM, Koplan BA. Incidence and predictors of major complications from contemporary catheter ablation to treat cardiac arrhythmias. Heart Rhythm 2011;8:16611666.
- Keegan R, Aguinaga L, Fenelon G, Uribe W, Rodriguez Diez G, Scanavacca M, Patete M, Carhuaz RZ, Labadet C, De Zuloaga C, Pozzer D, Scazzuso F. The first Latin American Catheter Ablation Registry. Europace 2015;17:794800.


{kind=link}